Need help with a complex symmetrical Teaching Hospital model
-
Charly:
The various versions (both schematic and 3ds max) of the 110m x 22m unit that I forwarded to you. This could seemingly represent our default unit. I attempted to explain the comparatively minor series of amendments that would need to be made to this in order to successfully convert it into a clinic. Maybe my explanations were rather poor ....
Please also read my earlier reply to mac1. Maybe (or maybe not) my comments might seem a little more clear ....
Perhaps (if mac1 is prepared to become actively involved with this project) you can forward him copies of your plans and models (as well as perhaps even my corresponding plans and models as comparisons) with any explanatory comments that you might feel are appropriate?
-
To put it into a more abstract question: how do you combine several skp files?
Well, once a file is saved in SketchUp, it can always be imported (and placed/aligned to your liking) as a component into a "master file" or model.
-
Another extremely relevant consideration:
How does one combine (collate for want of a better term) 2600+ of these already fairly large individual clinical facility modules (excluding additional non-clinical facility modules) into a composite main THC building?
This is the issue that currently worries me the most and will undoubtedly ultimately provide the greatest challenge ....
-
Hello Gaieus:
Great to hear from you ....

Thank you so much for that important piece of technical advice that will surely be employed when the individual modules are "collated" into the main THC model. However, my main concern is more aesthetic in nature - insofar as I am really keen to develop a truly striking main THC model (for the reasons previously mentioned) that will function as a detailed "walk-through" facility ....
This is going to prove very tricky indeed - especially as the various anatomical systems (18), clinical disciplines (65) and clinical subdisciplines (382) need to be rationally (systematically) grouped. Now this is what I would tend to refer to as process ....
-
Hello all:
Sorry for the repeated posts - but (as earlier stated) I am extremely keen to try to make some ongoing definitive progress with this most important aspect of our project ....
Upon deeper reflection, I think that a lot of our current misunderstandings can possibly be ascribed to our differing levels of process planning:
[*]On the one hand, Charly and mac1 (being experienced engineers) are looking at the lowest level details involving the microstructure and microfunction of the individual modules that will eventually be collated to form the body of the main THC. I fully understand and appreciate that this approach represents standard real world engineering practice and conventional wisdom.
[*]On the other hand, I (largely due to my complete lack of any engineering knowledge) am looking at the next level details relating to how the individual modules (both clinical and non-clinical) will structurally and functionally interact with each other within the body of the main THC. [Maybe it has been somewhat of a mistake and/or represents a major departure from real world engineering practice and conventional wisdom (although I tend to view it as more of a practical challenge) to initially propose a rather esoteric macrodesign for the main THC (especially as it is potentially hugely constraining) to house the circa 2600 (actually the final figure will ultimately be much nearer to 3000) modules].
I hope that there is a suitable (and possibly even highly innovative) way of overcoming this deep impasse as I sense that you are both keen to assist me and I dearly need whatever assistance that I can readily obtain with this most important aspect of our project. Does anyone have any ideas as to how we can proceed within (hopefully) the coming days ....

-
Jeremy,
What are you talking about 3000 modules, that's unrealistic. It is important to have a realistic basic concept as a starting point. Start with a small basic hospital. Later extensions are always possible.
The basic form of a hospital is, ideally, based on its functions:
- Bed-related inpatient functions
- Outpatient-related functions
- Diagnostic and treatment functions
- Administrative functions
- Service functions (food, supply)
- Research and teaching functions
Define the Services for each function which should be included as a minimum (but please, not 3000).
That would be a basis for further dicussions and we could then talk about further details and working steps.Otherwise you'll notice after a further six years you did not get a step forward.
Charly
-
Think you completely misunderstand. It is not uncommon for large( Yes I know yours will not be nearly this large) project to take maybe ten years from start too finish with many up front trade off designs to look at how one wants to accomplish the intended function(s). There will be many desing /schedule / cost studies etc. I think where Charly and I came from is the detail of the hospital vs how it fits in with the functions to be performed. You have targeted lay person and high school students in your original OP. So now what do you want to convey to them in your virtual world and what do you expect them to have when they get done with the simulation or tour? Also this will not be free so you must get funding form maybe some NPO OR ? and will need enough info to get the required help. At present I not not think you can submit coherent request to ask for a grant
 For example, if this would be used in a school setting or at home then you must consider what the target population has at their disposal to even participate. This leads me to the conclusion the building of the hospital model is the least of your worries and you are possibly( at this time ) dealing with the wrong technical disciplines. I guess I am saying you must first determine what the capability of the target population has at their disposal before you can go off and build something they can use. Based on you location I guess this maybe persons that do not have access to all the bells and whistles others may have. I am guessing you should be talking to some computer / network types => all system design folks? Once you can put on paper a top down functional requirement ( This is not a design requirement ) it comes latter then you can go to them. This will I am sure this will be an iterative process=> the more you learn the better you can refine.
For example, if this would be used in a school setting or at home then you must consider what the target population has at their disposal to even participate. This leads me to the conclusion the building of the hospital model is the least of your worries and you are possibly( at this time ) dealing with the wrong technical disciplines. I guess I am saying you must first determine what the capability of the target population has at their disposal before you can go off and build something they can use. Based on you location I guess this maybe persons that do not have access to all the bells and whistles others may have. I am guessing you should be talking to some computer / network types => all system design folks? Once you can put on paper a top down functional requirement ( This is not a design requirement ) it comes latter then you can go to them. This will I am sure this will be an iterative process=> the more you learn the better you can refine.
I am even thinking you are in the wrong forum for your effort
Sorry if I am still way off base -
Charly and mac1:
@unknownuser said:
What are you talking about 3000 modules, that's unrealistic.
This concept appears to work rather well in my (albeit rather simplistic) Schematic World Map (the relevant section of which appears as a screenshot in the MS Word document I forwarded to you containing the list of all the relevant clinical disciplines and their component clinical subdisciplines). I am basically exploring ways of presenting this information in a far more striking, dynamic and interactive fashion ....
@unknownuser said:
It is important to have a realistic basic concept as a starting point. Start with a small basic hospital. Later extensions are always possible.
While I suppose that we could do this (especially if you and mac1 are prepared to assist me with this process), I suggest that there is already a concept in place - the proposed taxonomy (classification) of 18 major anatomical systems, their 65 component clinical disciplines, their 382 component clinical subdisciplines and (finally) their circa 2600 dedicated clinical facilities (including 8 main component upgradeable structures).
@unknownuser said:
The basic form of a hospital is, ideally, based on its functions:
- Bed-related inpatient functions
- Outpatient-related functions
- Diagnostic and treatment functions
- Administrative functions
- Service functions (food, supply)
- Research and teaching functions
Now we are coming to the "heart of the problem" ....
Each clinical subdiscipline (generally) features the following clinical facilities (a clinic. a unit, a clinical diagnostic laboratory, a surgical operating theatre (where appropriate), a clinical research unit, a teaching unit, a scientific research unit and an intensive care unit (where appropriate)). Each clinical subdiscipline is well-defined (such as Adult General Cardiology which will include medical heart conditions affecting adults not relating to the other specialist adult cardiac clinical subdisciplines).
Therefore it should prove fairly simple to generate a series of fairly basic relevant functions for any one of the proposed 2600+ clinical facilities based upon either their type (clinic, unit, etc.) or clinical subdiscipline (such as Adult General Cardiology as quoted above). I really don't know what further details will prove necessary .... ??
@unknownuser said:
Define the Services for each function which should be included as a minimum
Please refer to my comments above.
I even provided you with possible staff lists in this regard - although I admit that they are still a little "exploratory" ....
@unknownuser said:
That would be a basis for further dicussions and we could then talk about further details and working steps.
I must admit (with all due respect) that I would hugely welcome some fairly definitive action ....
@unknownuser said:
Otherwise you'll notice after a further six years you did not get a step forward.
Well - this is not entirely true as my volunteer programmer is making some (albeit slow) progress with our all-important Schematic World Map. It is just extremely unfortunate that he has been affected by poor health for the past 6 months ....
@unknownuser said:
I think where Charly and I came from is the detail of the hospital vs how it fits in with the functions to be performed. You have targeted lay person and high school students in your original OP. So now what do you want to convey to them in your virtual world and what do you expect them to have when they get done with the simulation or tour?
They will (for absolute starters) know what each clinical facility does as each clinical discipline and clinical subdiscipline has been defined. The function of each clinical facility has been likewise defined. [We are also busy exploring a healthcare delivery model whereby healthcare services are delivered to the community on a major anatomical system-specific manner].
Depending upon what else can possibly be included within the virtual world, there might conceivably be other healthcare education opportunities within the main THC (which is only a part of the entire application) ....
@unknownuser said:
Also this will not be free so you must get funding form maybe some NPO OR ? and will need enough info to get the required help. At present I not not think you can submit coherent request to ask for a grant
I fully realize this - hence the relative urgency in my quest to create a high-impact "flagship product". However (at present), everything has been created by a series of selfless volunteers ....
@unknownuser said:
I guess I am saying you must first determine what the capability of the target population has at their disposal before you can go off and build something they can use
The model would obviously have to be fairly easily integrated into our default application. Otherwise, I suppose that it could represent an optional "extra" that could be used (by some) in conjunction with the essentially rather basic default application (which was of some interest to the local Education Department) ....
More in follow-up post ....
-
SUMMARY:
I am beginning to wonder whether this concept of a fairly detailed main THC model (whose components are directly linked to the content of the Schematic World Map) is possibly a "bridge too far". I certainly don't seem to possess the ability to provide Charly (in particular) with the depth of details required. However (to be absolutely honest), I really don't think that most of these seemingly highly detailed processes are currently relevant to the envisaged nature (and scope) of our application. Maybe (with the passage of time and successful completion of the absolute basics) it might eventually prove possible to successfully fill these gaps ....
I see our application slowly growing from a fairly humble beginning into (hopefully) something ever more detailed. However, I honestly feel that we need to initially build a solid (albeit somewhat basic) foundation before adding a huge amount of (presently unnecessary) technical data. Hence my analogy of a "bridge too far" ....
I would really love to work with you two highly-skilled professionals - but you are going to have to substantailly lower the proverbial bar for this non-engineer. Otherwise we will forever be talking at cross-purposes and wasting all our time. This would be really sad - but I am well-aware of this risk ....
-
Jeremy, very simply put: the dreams and details you want to squeeze into this giant monster will inevitably constrain any skp model to a freezing halt. You can either imagine and dream of an exterior view of this complex OR some separated files with details when it comes to all the medical equipment put into a single department of this THC.
You will neverbe able to see the whole thing together in SketchUp. It is too much for it.
-
Hello Gaieus:
Yes - I have sadly come to the same conclusion ....
However, you do raise two interesting possibilities that might potentially release us from some of the emphasis on process:
[*]I am still extremely interested in a fairly detailed exterior view of the proposed "twin wing" and "twin ring" model (as iirc appears on page 1 of this ever lengthening thread). However, I am not too sure whether either mac1 or Charly would ever be prepared to even attempt this rather fanciful design (with minimum emphasis on process). I still feel that a suitably well-crafted model would provide us with a wonderful centerpiece to showcase our application ....
[*]I have previously discussed a series of fairly simple templates for the nine different types of clinical facilities with Charly. However, this discussion has become increasingly "bogged down" with references to process. I am basically looking for a series of fairly simple (but well-crafted) designs that can possibly be inserted into our Schematic World Map.
Maybe I place too much emphasis on appearance over form - but I am somewhat desperately looking for suitable content to complement our Schematic World Map. I now see that the "monster" I initially envisaged is just too large, too ambitious and too impractical ....
Hopefully I have not "chased" Charly and mac1 away with this impossible idea. However, I do need something reasonably definitive sometime soon. Therefore I entreat them to seriously consider undertaking some creative modelling on my behalf. I have already seen the high quality of Charly's work and somehow suspect that mac1 is equally adept ....
-
You don't need to model the entire thing in detail inside just one giant SKP file - which would become unbelievably unwieldy...
You can make a relatively simple 'external model' to show the massing and the relationship of the 'parts' to each other and the site.
The 'parts' can be modeled as separate SKPs.
Many of them will be similar - e.g. a few ward-types will suffice for most...
If you are making a presentation you can splice the different SKPs together so the viewer just assumes it's one continuous thing...
So like with everything on this project you need to 'plan'.
Plan the relationships of the parts.
Plan the building.
Plan the parts.
Plan the 'modeling'...

I'm out... -
Hello TIG:
Thank you so much for your sage input.
I am indeed looking for someone who is prepared to actively assist me with developing the exterior model. I fully realize that this process will not only require fairly intricate planning (which does not represent my strong point) but also a fair amount of time in execution.
[Sandy and I spent several months working on the comparatively simple "single winged" and "single ringed" THC model. I have compiled an extremely lengthy (and somewhat confusing) transcript of the most relevant correspondence we conducted during this period. There are therefore some details regarding some of the features that could (should) be included in the exterior of this proposed model. There is also significant scope for much further embellishment - so that the modeler could quite feasibly impart a great deal of themselves into this model].
I just need to find someone who is prepared to attempt this fairly complex task ....
-
@sonofmoose said:
...I just need to find someone who is prepared to attempt this fairly complex task ....
Hi Jeremy, I've followed this and previous thread (starting about one or two years ago on Google sketchUp Help forum) and I'm just wondering.... couldn't this person be you yourself? You've spent so much time trying to explane the "rules" to put this health center together. I'm 100% sure that you could have modeled the whole thing together long time ago by just asking questions about how SU works.
Taking into account that SketchUp is a fairly easy to learn program and since you already know exactly what you are after, I'm sure you can do it with some help of us.
I'm not prepaired to model this THC but I'm more than willing to answer SketchUp questions to get you there, like many others here I guess. -
Hello Wo3Dan:
I have actually previously tried to master Google SketchUp but sadly possess extremely poor 3d perception. This disability has already not only caused me to repeatedly fail the yard test component of my drivers test but also caused me to struggle with all forms of venisection (thereby effectively blighting my clinical career) ....
I am still (seemingly against all sound judgement) hoping that a master modeler might either take pity on me and/or be sufficiently motivated by the challenge presented to offer their services to our project.
In all truth, this model does not represent an indispensable component of our proposed application - although it would surely add much value to it. It is therefore a much-cherished luxury that could (as previously suggested) function as a showcase centerpiece for it ....
I know that many Google SketchUp masters love to model real life buildings. Maybe one of them might instead be prepared to try to create something unique ....
In summary, you are also most correct in your comment that I have indeed spent a great deal of my time trying to (seemingly unsuccessfully) explain the "rules" (a good term) defining the proposed main THC. Unless I can soon find someone who is prepared to actively assist me in this regard, I think that it will be time to consider closing this already rather lengthy thread that has ultimately (and sadly) delivered nothing.
I was obviously hugely lucky to have managed to acquire the services of Sandy to create the "single winged" and "single ringed" model adorning the first page of this thread ....
-
I agree with Wo3Dan, your explanations of what you want don't really come together in other peoples heads and I'm sure you would see it all better if you modeled it yourself.
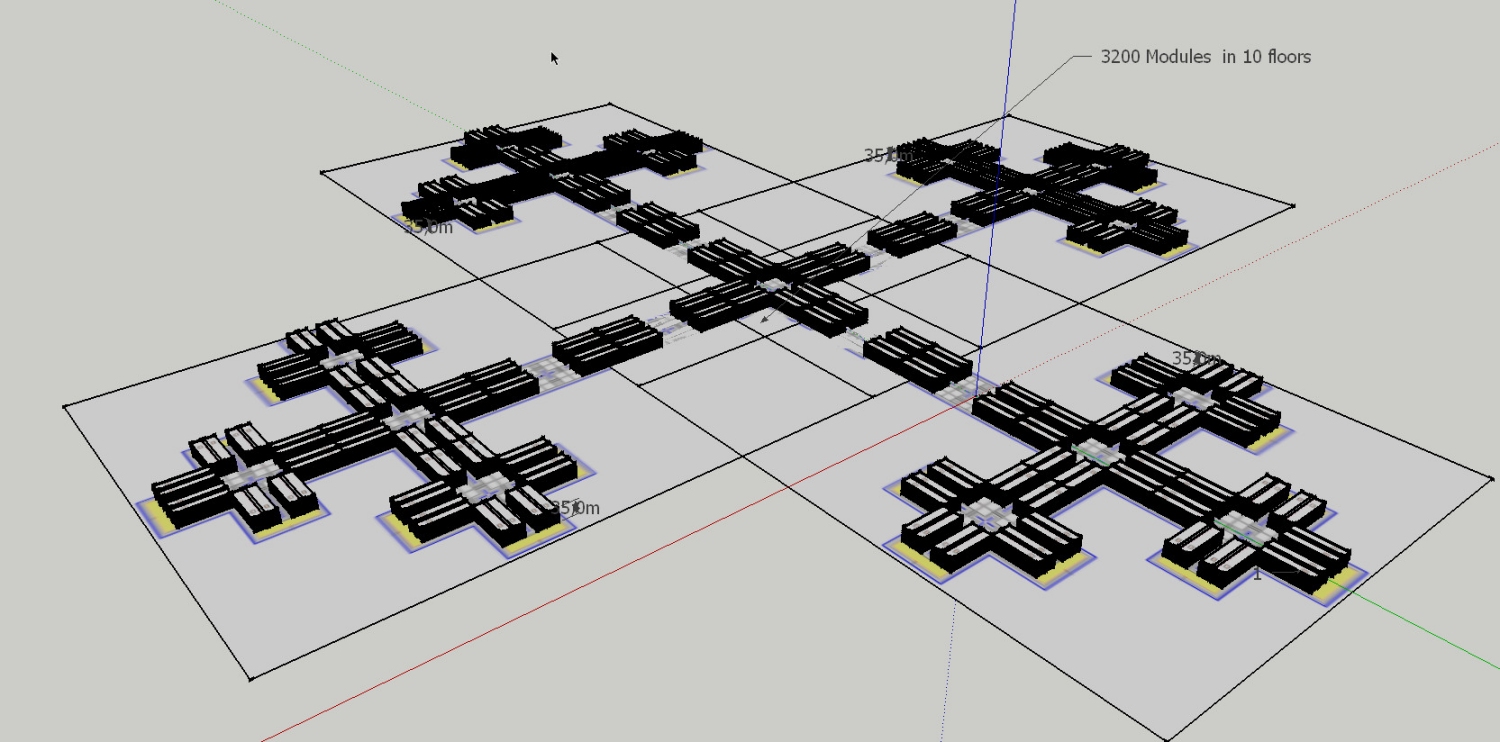
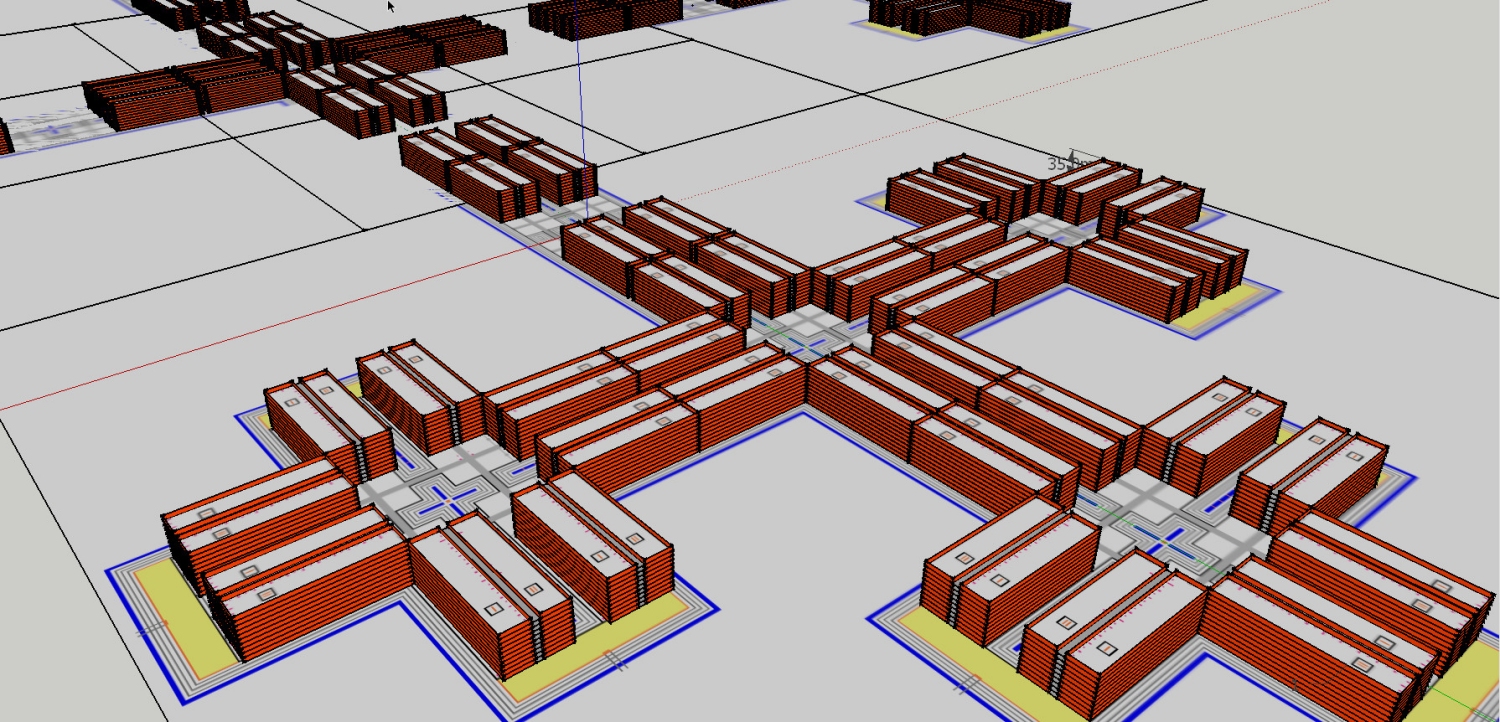
For example, I took your 100m by 22m with 6m corridors, modular structure and gave it a 3m high wall, as you will see from the attached image and skp file, the overall scale doesn't impress, it's too flat. It does however give you over 500 individual modules, some of which are naturally smaller and cut off by the design.
I only did this out of curiosity in a spare moment, I'm not interested in taking it any further.
-
Hello Box:
I am really impressed with your obviously fairly hastily designed model of my proposed main THC design. While not perfect in the positioning of the individual modules, it certainly does provide one with a good idea of what it could like at a slightly different scale.
I see that it has already had (iirc) 27 downloads. Is there anyone "lurking" in this thread who would like to try to "run" with this?
Otherwise I suppose that this might (quite possibly) represent a somewhat appropriate final post for this lengthy and ultimately vainglorious thread ....

-
Hi there:
Unless something truly meaningful transpires, this will most probably represent the final post of this thread.
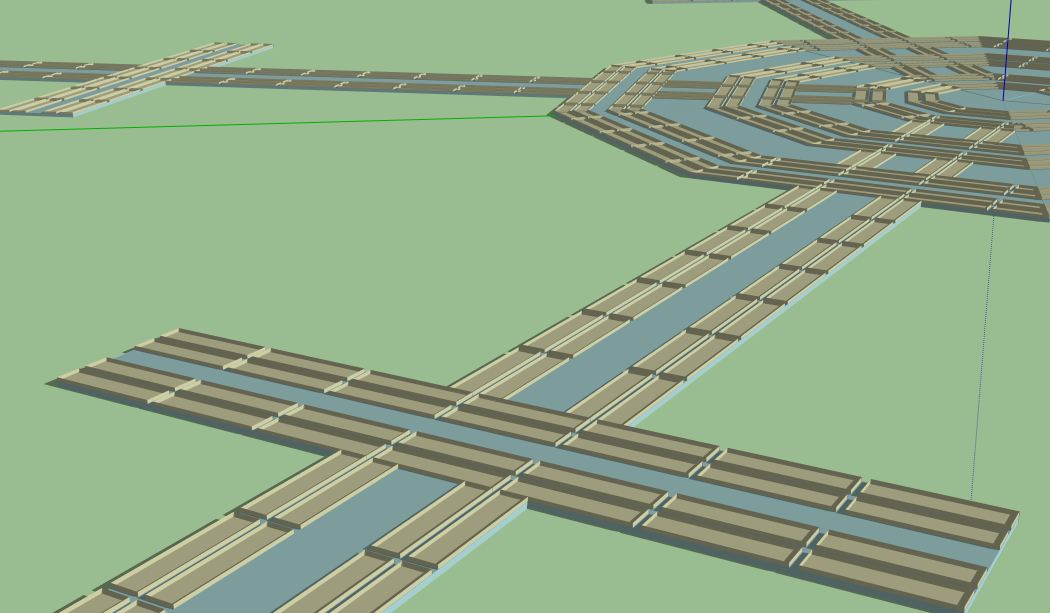
I have taken the liberty of attaching a (reduced size to meet the requirements of this forum) schematic outline of one of the five identical "double wings" (where each labeled rectangular block is a 110m x 22m module).
I would like to forward my kindest regards and sincerest gratitude to those people who have contributed to this thread.

The above outline placed within Google SketchUp
A slightly more complex (at the base) outline placed within Google SketchUp
-
-
Hello Charly:
You are certainly getting a bit closer ....
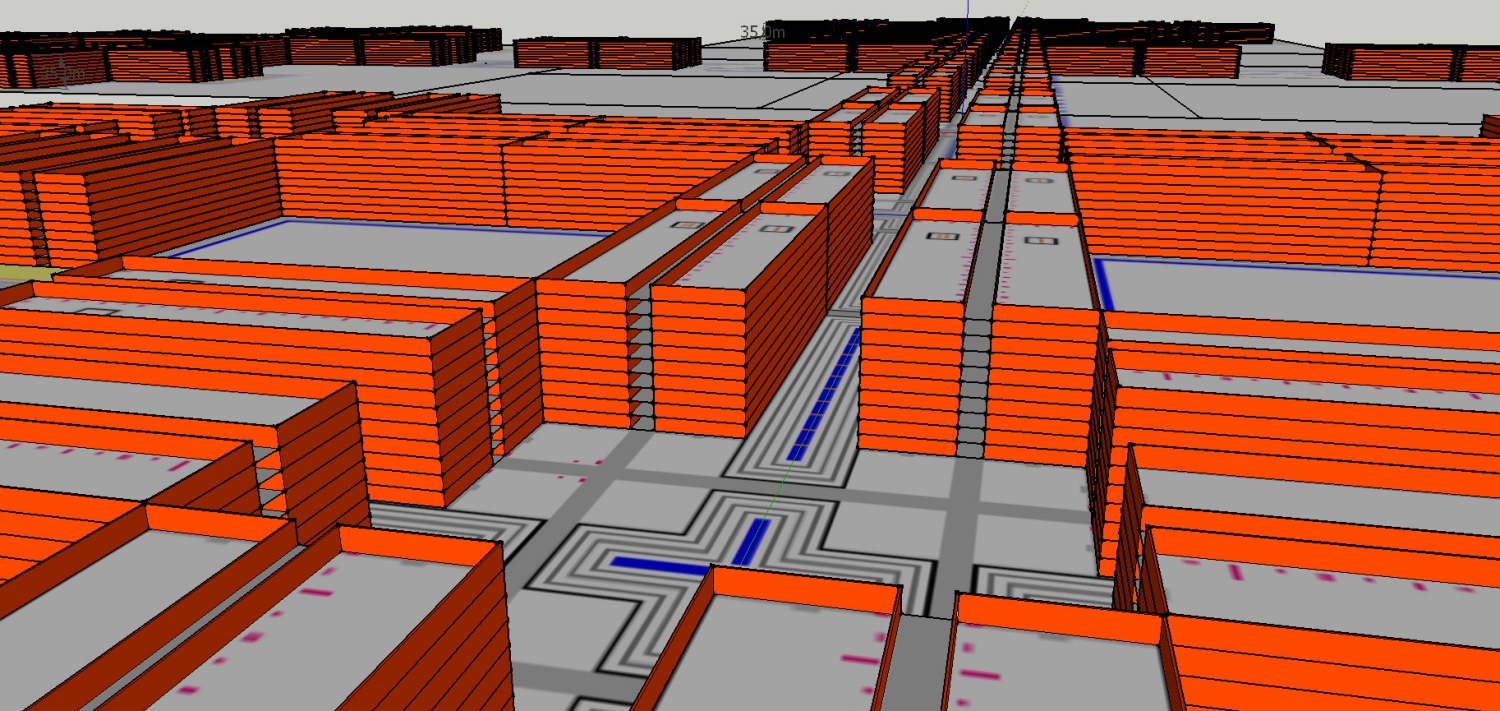
Unfortunately a 2d outline (of only one wing) does not easily translate into a fully-fledged 3d model of the entire complex (which consists of five identical wings and the central rings). For instance, the series of (presently flat) square shaped areas situated between the sets of modules are actually internal quadrangles (open spaces) that need to be enclosed within each floor. The internal passageways will also need "cut across" the internal water features (as a series of perspex-lined structures).
Maybe you can try these (fairly minor) modifications and we might (hopefully) slowly move forward ....

Hello! It looks like you're interested in this conversation, but you don't have an account yet.
Getting fed up of having to scroll through the same posts each visit? When you register for an account, you'll always come back to exactly where you were before, and choose to be notified of new replies (either via email, or push notification). You'll also be able to save bookmarks and upvote posts to show your appreciation to other community members.
With your input, this post could be even better 💗
Register Login







Advertisement