Need help with a complex symmetrical Teaching Hospital model
-
Hello Brodie
Thank you so much for your latest reply.
You are indeed asking some hugely relevant questions that most definitely need to be adequately addressed. I am (at the very least) looking to develop a freeware healthcare education programme initially targeted at local high school students interested in pursuing a career within the Healthcare Sciences (although it should also appeal to anyone with an interest in the structure and function of a modern healthcare system).
The flagship of this project will undoubtedly be the main Teaching Hospital complex (THC) because of its sheer size and complexity due to the wide range of clinical facilities contained within it. At the moment (largely due to its enormous size), it is being depicted in an entirely abstract fashion within our Schematic World Map.
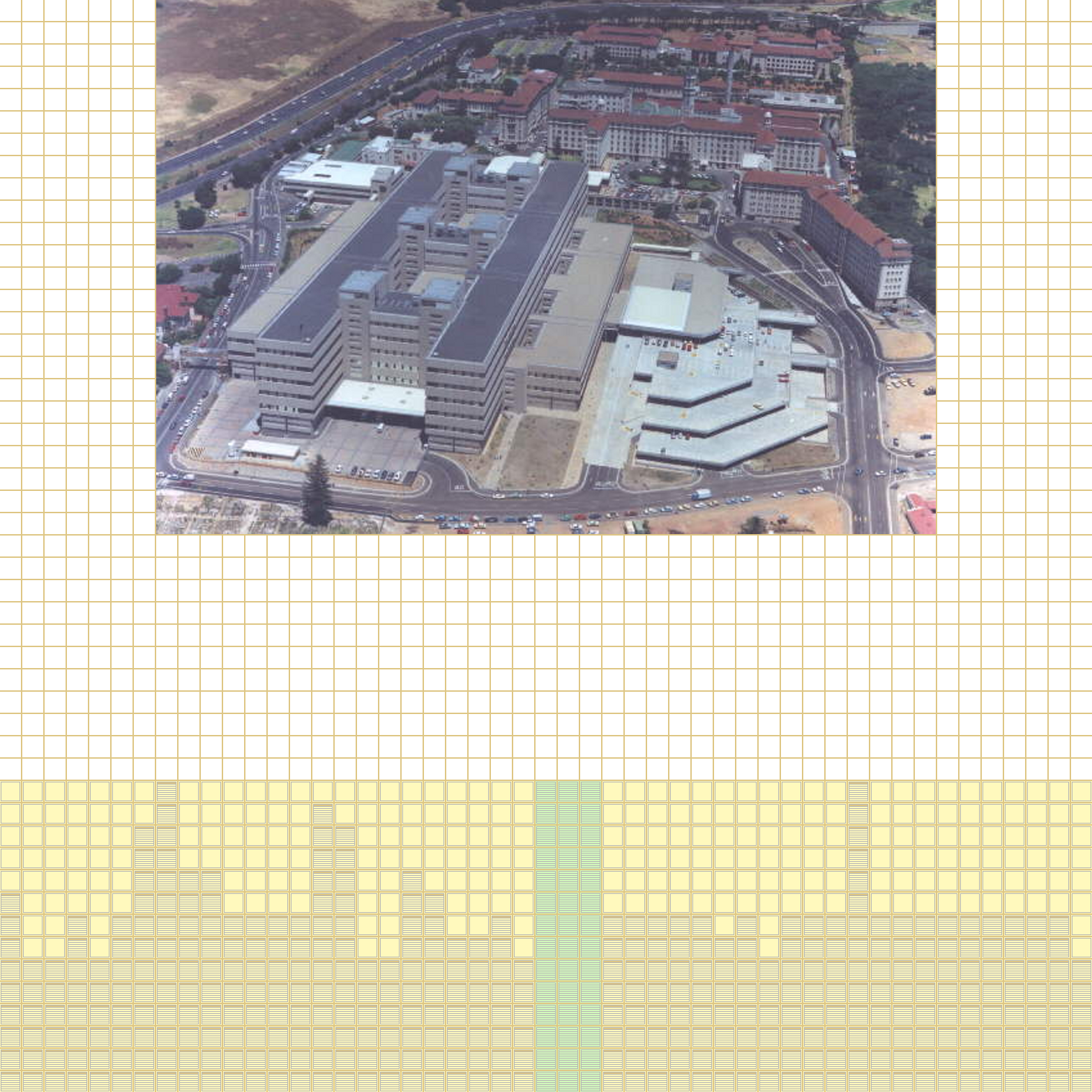
Each of the yellow vertical columns below the image of Groote Schuur Hospital (24 + 22) represents a specific clinical discipline based upon 18 anatomical systems. Each individual striped tile featured within each of these 46 columns represents a specific clinical subdiscipline. Each clinical subdiscipline will generally consist of seven or eight clinical facilities. Therefore there is a titanic amount of detail contained within the main THC.
Each clinical discipline, clinical subdiscipline and clinical facility will be described and explained to the user. This might only represent the beginning of the educational process.
While (in some respects) the abstract schematic approach might potentially work better, I am convinced that the use of suitable (preferably high quality) architectural models would serve to greatly enhance the quality and ultimately success of the envisaged product. I would be most happy to actively discuss all relevant ways of upgrading our purely schematic application into something far more striking.
Above is an earlier version of our Schematic World Map showing the central position of our main THC. There will be eight much smaller Secondary Hospitals (SHs) positioned around it. Each SH will have multiple Primary Healthcare (PHC) clinics situated around them.
Even at the most basic level, a degree of interactivity between these various healthcare facilities is envisaged. At a more advanced level, various healthcare variables could be added in order to hugely enhance this ability.
I am not too sure whether this diatribe adequately answers your "WHY" - although it does possibly add somewhat to the "WHAT" ....
-
Indeed, you've clarified the "what" further. It's a standalone freeware software containing an entire healthcare system.
And the "who." It's for anyone wanting to learn more about the structure and function of a healthcare system.
Now back to the "why". Perhaps some more specific questions would help to flesh this out.
-
Why a theoretical idealized system rather than a real world system. Why not just take a system like Catholic Healthcare West and illustrate how it runs, what it's hospitals are like, how they're interconnected, etc.?
-
Will the users be able to literally walk through the model? If so, shouldn't it be based on real world rules like concern for departmental adjacencies and circulation space? If the user can't walk around then why not just model the individual rooms where the user can navigate without modeling circulation, exteriors, etc.?
-
Why freeware? Why not make money for the time and effort?
-Brodie
-
-
Brodie:
Although the healthcare system is presently somewhat theoretical and idealized (one has to start somewhere), I am trying extremely hard to base it upon the local (anything but idealized) system. I live in Cape Town (South Africa) where healthcare service delivery is in a major crisis. To state it somewhat bluntly, there are way too few healthcare facilities (especially at the primary level), far too few healthcare professionals (workers) and (correspondingly) way too many patients. Apart from anything else (and I freely admit that this is potentially extremely naive), I strongly feel that local people should know what is considered as appropriate (not even ideal) to their needs ....
Lets just say that the local healthcare system is severely damaged ....
As for the amount of user interactivity offered. That will obviously (as always) dependent upon the amount of voluntary assistance that I can obtain in this regard. I would certainly strongly desire the ability for the user to be able to literally walk through the various healthcare facility models. I feel that this would not only add immensely to the overall value of this application (as presently perceived) but also potentially provide multiple avenues for future expansion ....
[At present separate rooms depicting the huge number of individual clinical facilities are perceived. There will obviously only be a handful of template designs (mainly for each type of facility). They will be separately linked to the Schematic World Map but will obviously not be interlinked to each other within a separate main THC (SH or PHC clinic) model. A separate main THC (SH or PHC clinic) model (as a replacement for the various healthcare facility images) would surely represent the proverbial "Royal Road" ....].
Btw: Verisimilitude will be key to this project. However (for the reasons stated above), I have little reason no wish to replicate the conditions prevalent within our public healthcare system (although it could be ultimately be possible to "chop-and-change" the number and quality of existing healthcare service facilities) in order to simulate different types of service delivery ....
I strongly feel that this information should be freely available to the public - especially to the school going children of historically disadvantaged people who still live under a heavy burden of inadequate housing and disease. As I am currently unemployed (and looking after my 88 year old Alzheimer's affected mother in-between working on this project), I do intend to try to seek sponsorship (both personal and for the project) once something more meaningful (i.e. more content) has been created ....
-
If you don't mind I'll reply both to your post as well as your private message here as it's probably beneficial for anyone coming along later and reading through this to have all this info in one spot.
In response to your question about where I'm from, I'm from the United States. I gather that your healthcare system is more publicaly funded? We have some publicly funded hospitals here but most tend to be run privately, mostly by religious organizations.
Your project certainly sounds interesting and I could probably continue asking questions for a long time to come but I think you've answered most of what I've asked pretty well. Do to a busy schedule I can't make any real promises about how available I'd be but I'm at least interested to see what exactly you'd want me to work on. Do you have any specifics as to what the next step is that you'd want me (or someone else like me who may be reading this) to work on?
-Brodie
-
Brodie:
We possess an excellent private healthcare system that serves the less than 20 per cent of the population that can afford it. Sadly (as previously intimated) the public healthcare system is meant to service the remaining 80+ per cent of the population (including virtually all our historically disadvantaged communities). Therefore it is not too difficult to see the huge disparity that presently exists between the private and the public sectors with respect to the quality of services offered.
As stated in my PM, this regrettable but inescapable fact is one of the main reasons that motivates my interest in this project ....
I suppose that there are two potential areas in which you or any future volunteer could work:
In developing a series of related outlines for the main categories of individual clinical facilities (such as clinics/outpatients departments, units/wards, clinical diagnostic laboratories, etc.). I already have a fairly good outline for a unit/ward in Google SketchUp (previously developed by a volunteer architect) that could hopefully be further refined.
(In many respects I now hesitate to ask) - but in developing an outline for the main THC. As previously mentioned, I have a less complex version of it in (iirc) 3ds Max 2008 format. Maybe it could at least somehow be used to showcase our still rather bland and basic product?
In many respects, I need further advice as to how precious voluntary architectural services could be best used to advance our project which is (in itself) a genuine attempt to uplift (the healthcare knowledge of) historically disadvantaged communities.
We really do need as much assistance as we can obtain ....
-
Perhaps you can post one or both of the files for users here to take a look at. Maybe post them through dropbox ( http://db.tt/j2IZMoG ) or something similar. That'll give me, and perhaps others, a chance to get familiar with what you already have and perhaps take it to the next level. If you post the .max file I can convert it to sketchup for others to open up.
-Brodie
-
One might need to initially import the attached (zipped) 3ds Max 2008 file/s into SketchUp version 6 in order to obtain a functional SU file which can then presumably be updated to the latest version of SU.
If anyone is genuinely interested in becoming voluntarily involved in this potentially most meaningful project (by taking the attached file/s to the next level of functionality), please PM me. Although this forum is an excellent resource for exchanging ideas and work files, it will probably prove much easier to ultimately develop an e-mail based "relationship" outside of this venue ....
I truly look forward to receiving some feedback - either in this thread or via a PM ....
Zipped copy of latest 3ds Max 2008 THC (old style) design
Zipped copy of a slightly earlier 3ds Max 2008 THC (old style) design
Zipped copy of 3ds Max 2011 proposed THC typical ward design
-
Sorry for the bump - but hopefully someone might possibly be interested in doing something with the attached files and slowly pulling this project forward ....
-
Hi Jeremy,
Would it be possible to post the files in 3ds format. As far as I know you can only convert max files with 3DS Max in 3ds files.
Charly
-
Hi Charly
Herewith are attached the two 3DS Max files exported as two 3ds files ....
-
Charly:
Please let me know (possibly via PM) whether you have had any luck with viewing the above files and what you think of them.
I really need your ongoing assistance if you are sufficiently interested to assist me with this extremely ambitious design ....
-
Any other possible takers?
-
@sonofmoose said:
Hello
"I am a registered medical practitioner with a research Masters degree in Psychiatry and Mental Health who is extremely interested in the ability of computers to play an important role in both professional and lay person healthcare education. As a direct result of this interest, I have been working for the past six years on my proposed freeware healthcare education application (simulation) that is initially aimed at high school students."
Not in healthcare field nor architecture but have done technical management of 1/2 billion dollar programs. As you are well aware form follows function and I see your goal above but suddenly find you in the detail of the structure design, water features, parking grages etc. with a considerable time elapsed and I ask my self the question are you stove piped ? I see no relationship to the following discussions and your goal above. I may be worth your time to set down and draft a spec. or specs ( In this case it would be a software or model requirements ). My contention is your goals can be more quickly obtained by possibility a number of modules vs trying build a very complex initial model. Once those basics are done then the integration of those into a much larger model can be done on a timed sequenced basis?
Sorry if I am completely off the mark but I think your lack of progress, the number of questions and vol. support etc. some what supports my thoughts.SoM [Jeremy]
-
Hello mac 1:
I have sent you a PM largely agreeing with your sentiments and requesting possible assistance. Perhaps we might be able to "take things a bit further" ....
[Btw: I would love to hear from you again "Charly2008" .... ].
-
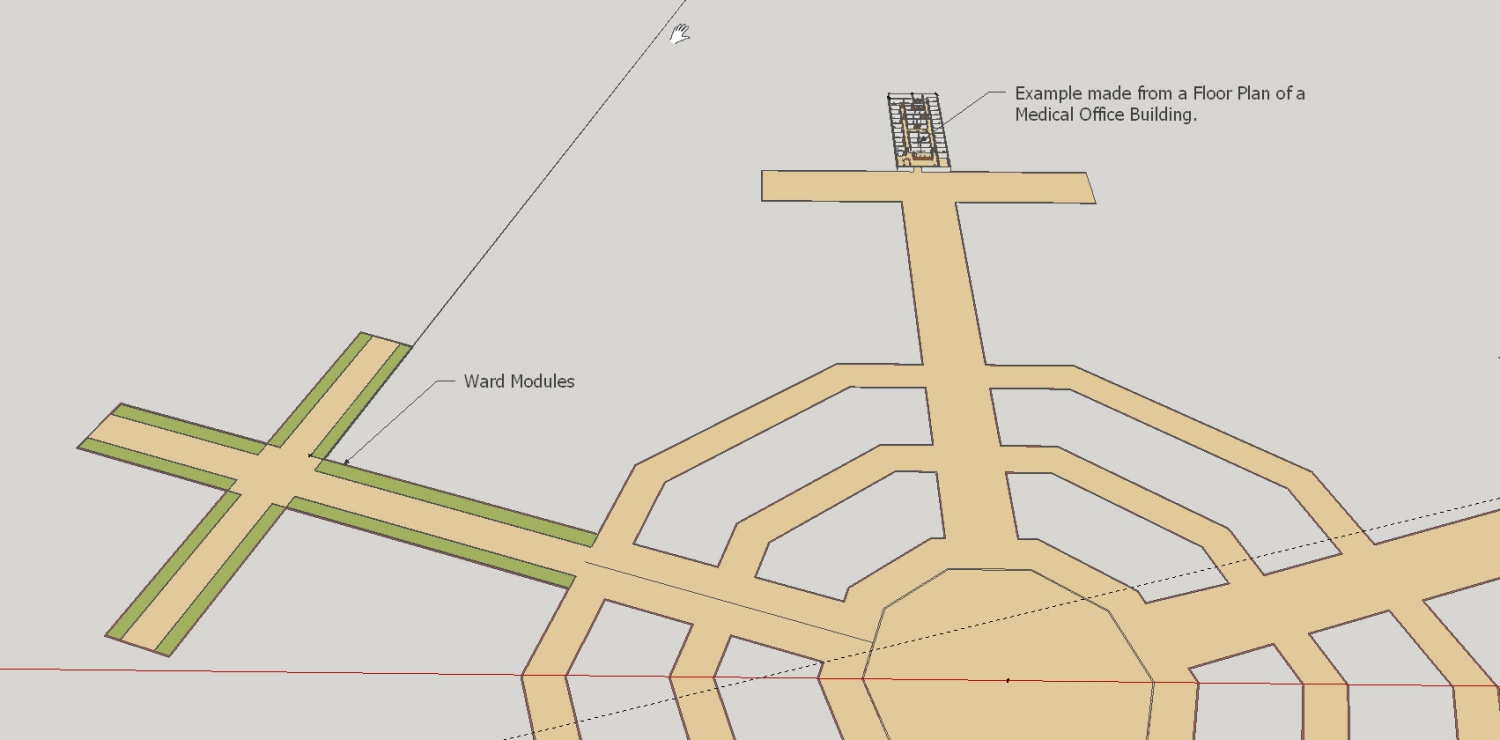
Each clinical facility is currently envisaged as 110m in length and 22m in width. Separated by a 6m wide central passageway, these parallel modules (for want of a better term) permit a 50m wide wing.
Maybe there is a suitably skilled and adventurous modeler who might be prepared to assist me in developing a conceptual version of the proposed macro THC model by examining how to lengthwise accommodate a series of these modules (together with cross passageways for access) into the complex symmetrical design .... ??
-
Hi Jeremy,
any reasonably talented modeler is able to incorporate your 110 x 22 m wide modules into in a floor plan. But where is the sense if you do not know what will occur in these modules.
I'm still not clear what you want to show with your simulation. If you want to show real processes in a hospital you have to orient yourself even in real processes.
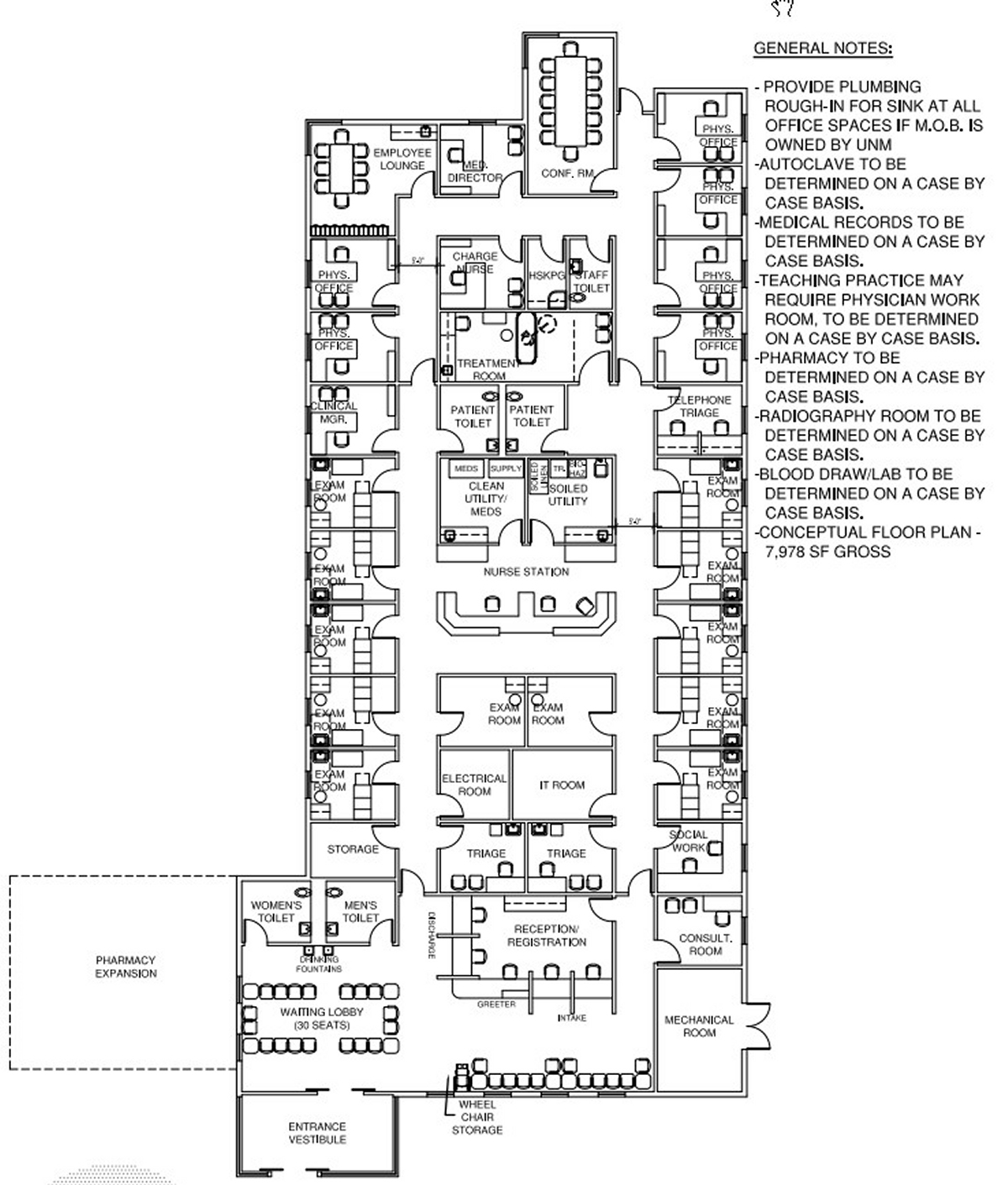
The first step would be to specify what should be shown in the model or Modules and how detailed it should be. What medical disciplines should be represented. Then you could perhaps take exemplary floor plans of existing clinics as the basis for the development of the model.
For me it makes no sense to construct a gigantic building and then think about how to fill it. I've looked at your so-called Ward module. A 110-meter walkway with rooms on the right and left side of the walkway. The rooms show some hospital beds. The ceiling height is about 4.5 meters and the thickness of the outer wall is 1 meter. What will you do with it? Of course, one could fill the whole building with these modules, but what should the aspiring physicians to be shown?
You can even ask your Ward module for discussion here because I'm just a simple mechanical engineer. Perhaps there are experts in the forum who are familiar with the hospital planning.
Charly

-
Hi Charly:
It is really good to hear from you again ....
At the moment, I am keen to see how a series of equally-sized modules would fit into the proposed macromodel. [This being the far more complex "double winged" and "double ringed" structure modeled on page 1]. I do (with the utmost of respect) believe that we are seemingly becoming unduly "bogged down" with all of this emphasis on process. I fully understand (from both you and mac1) that these are (quite understandably) vitally important (real world) engineering principles. However, I am looking at this issue from the (virtual world) medical educational perspective - where all these clinical facilities (and their component functional structures) will be labelled and fully explained (but most likely in less professional engineering terms) to the user ....
The 110m x 22m unit (which can easily be converted to a clinic) plan includes (imho) all the major functional structures required for both of these clinical facilities (independent of their clinical subdisciplines) to function (optimally). Maybe (with the passage of time and the considered expert input of a super-specialist hospital designer) the design can possibly be further fine-tuned. However, we do have something "concrete" with which to work and move forward ....
For various reasons, I am growing increasingly keen (desperate) to move forward with this aspect of our much larger project. [You are already in possession of the extensive list of clinical disciplines and clinical subdisciplines that will be housed within the main THC. We surely have the framework to attempt to push forward with this now ....
I strongly urge you and mac1 (as well as anyone else who has the time and inclination to become involved) to assist me with the ongoing development of this model. Admittedly (from the viewpoint of both of your professional training) we will be approaching this task "back-to-front". Please put these concerns aside for a while and see how we can "move forward" with this exercise. We will often be "flying by the seat of our pants" but I believe that we already have a sufficiently strong foundation upon which to build ....
Would the two of you be prepared to work together with me? The time zone difference between the two of you could be made to work strongly in our favour ....
-
Sorry I have to again state form follows function and your previous statements you don't have any budget restrictions is not correct. You have seen AVATAR I guess and they probably spent millions if not hundreds of millions for software, programs , hardware etc. I just cannot rationalize you stated goals on the OP with this obsession with the hospital layout when there are really more pressing problems than it. If you are going to make your project a success then spending time to decided what functions are really needed and a schedule so people asking all the questions can really understand what is required. Is your goal to teach the high school students how to park in a hospital, find there way around one ,or have some type of medical science simulation that they can step through and learn something. Are they off site or in one location and will you be using existing simulations, programming as part of this or just what?
Sorry as you can see you have yet to convey your concept to me
Front to back or back to front has no meaning to me expect your are heading for diaster -
Hi Jeremy
However, I am looking at this issue from the (virtual world) medical educational perspective - where all these [b]clinical facilities (and their component functional structures) will be labelled and fully explained[/b] (but most likely in less professional engineering terms) to the user ....But please, please give us a small practical example where we can see how that should look like! My imagination is not enough to understand this.
Charly
-
Hi mac1:
Well - from the point of software, I effectively have zero budget. I am currently an unemployed person trying somewhat desperately to make some beneficial use of his spare time (when not acting as a geriatric caregiver).
Maybe my obsession with the hospital layout is indeed somewhat inappropriate - but I am looking for a suitably high-impact centerpiece (with a high OMG factor) for our application. There is a fairly well-known maxim that "graphics maketh the game". Our Schematic World Map (which is presently envisaged as the core of our application) currently features extremely simplistic graphics (as created by me). The main THC model is meant to complement (and possibly eventually augment) the series of Schematic World Map tiles representing (in a largely abstract fashion) the individual clinical subdisciplines.
The main purpose of this part of our application could largely be stated along the lines of "finding ones way around the hospital" and explaining the function of the various clinical subdisciplines. I don't presently envisage developing a detailed medical science simulation as this is the property of large university research departments (such as Stanford University). Therefore the underlying purpose is actually rather simple - although I would like to include a fair amount of detail within this model to show the major components of a clinic (outpatients department), unit (ward), etc. [I have already listed these as a series of potentially upgradeable structures].
I am hoping that the user will be able to "walk through" the complex (which can feature a large series of explanatory labels as well as links to the relevant tiles featured in our Schematic World Map). Although I am hoping to eventually develop a healthcare systems simulator, it will not (at least for the foreseeable future) feature any detailed clinical simulations. This is somewhat outside my relevant area of expertise and (as stated above) there is no way in which I can even think of competing with the current major players in this area. However, an application featuring a large (and suitably detailed) main THC (without clinical simulations) appears to represent a more unique concept (especially when it forms an integral part of a greater healthcare system) ....
Therefore the concept is seemingly strongly based upon macro-design rather than overly on process. I am especially interested to see how all the individual clinical (and non-clinical) modules can be functionally arranged within a macro-complex. [Maybe the proposed main THC model can be "ditched" for something more sustainable .... ].
I hope that I have not severely disappointed you with this answer. Maybe it does (hopefully) more accurately explain my seeming obsession with the macro-design. Please (maybe with Charly) try to help me as best as you can to achieve my stated goal (and maybe any others that might follow from this) ....
Hello! It looks like you're interested in this conversation, but you don't have an account yet.
Getting fed up of having to scroll through the same posts each visit? When you register for an account, you'll always come back to exactly where you were before, and choose to be notified of new replies (either via email, or push notification). You'll also be able to save bookmarks and upvote posts to show your appreciation to other community members.
With your input, this post could be even better 💗
Register Login







Advertisement